|
LecturesPreviously Failed CRT Cases Implanted Successfully Using a Guide Support Based Telescoping CRT Delivery SystemWorley, SethIntroduction
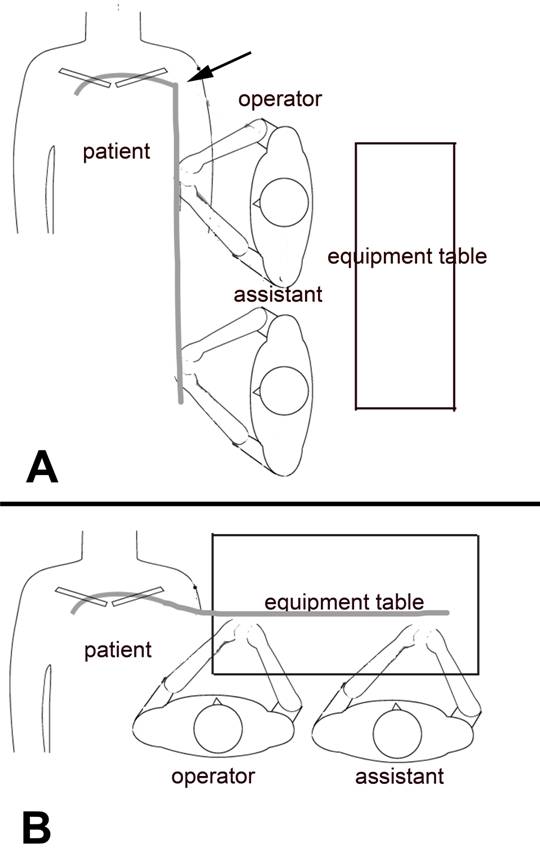
Figure 1. Table positions at the time of device implantation. In panel A the equipment table is in the position suitable for implantation of the RA and RV leads. When implanting the LV leads turning the table to the position illustrated in Panel B improves the ergonomics. The assistant is in a better position to help. The catheters are not kinked (arrow) as they would be if the table is kept in the position shown in Panel A.
Case Report #1
Figure 2. At Initial coronary sinus (CS) access was obtained with the 9F SafeSheath CSG® Braided Core Worley-STD® anatomically-shaped, peel-away sheath (sheath). (Pressure Products San Pedro, CA USA)
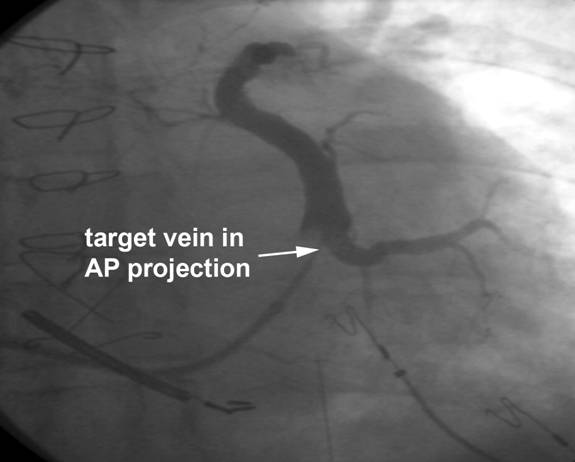
Braided Core Worley-STD® anatomically-shaped, peel-away sheath (sheath). (Pressure Products San Pedro, CA USA) Occlusive CS venography was performed in the LAO, RAO and AP projection (Figure 3) and the target vein attempted at the other institution was identified.
Figure 3 Occlusive CS venogram from case 1 demonstrating the lateral wall target vein
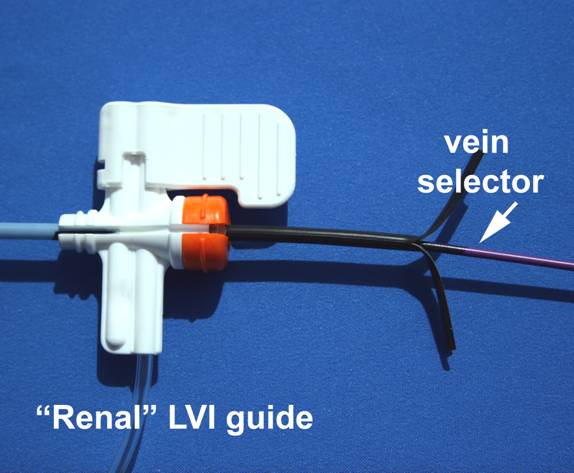
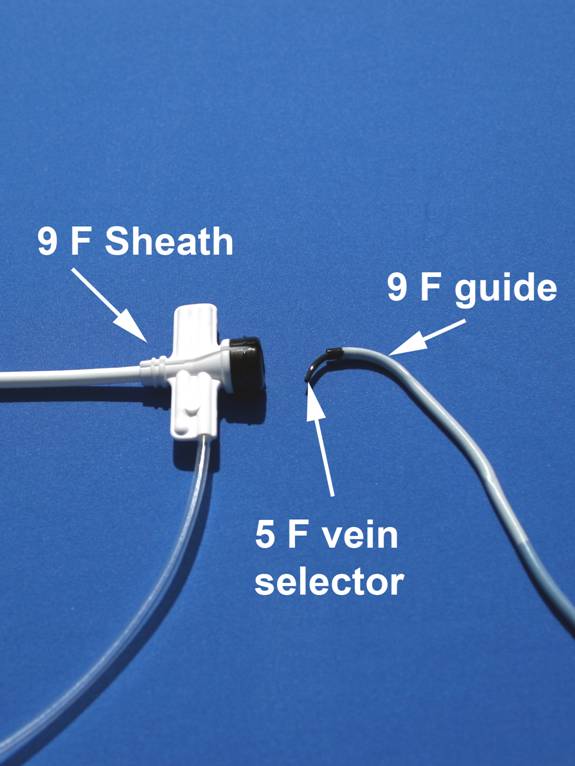
AAs shown in figure 4 a 5F vein selector was inserted into a 9F outer diameter (OD) 7F inner diameter (ID) preshaped renal curve braided catheter with break away hemostatic hub (Pressure Products SafeSheath® Worley Telescopic Braided Series Renal Lateral Vein Introducer® ) (“Renal” LVI guide ).
Figure 4 The 5 F vein selector is inserted into the 9 F SafeSheath® Worley Telescopic Braided Series Renal Lateral Vein Introducer® (9 F “Renal” LVI guide). (Pressure Products San Pedro, CA USA)
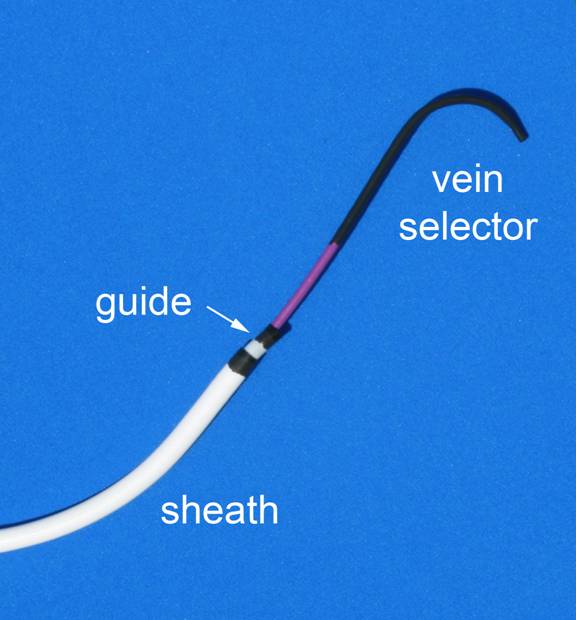
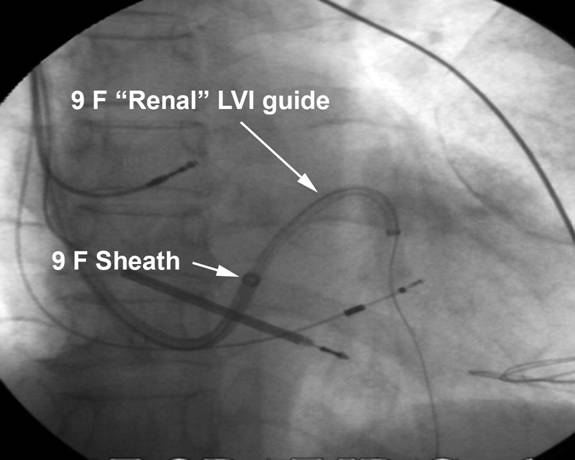
The “Renal” LVI guide containing the vein selector was inserted into the sheath (Figure 5) the telescoped through the 9 F peel-away sheath into the CS until the tip of the “Renal” LVI guide was at the tip of the sheath.
Figure 5 The vein selector/LVI guide are inserted into the long 9 F sheath located in the CS.
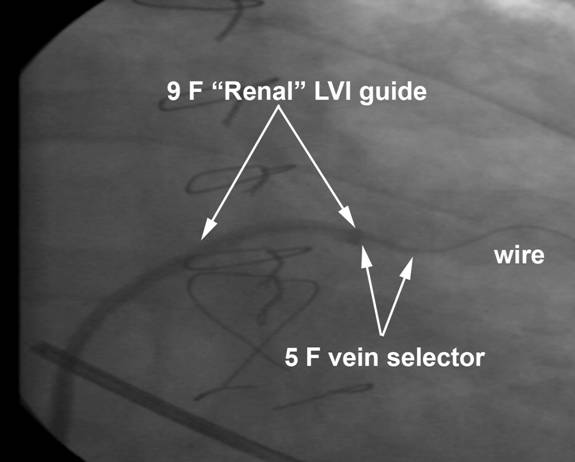
The vein selector was then advanced out of the “Renal LVI guide into the CS (Figure 6).
Figure 6 The sheath, vein selector and “Renal” LVI guide shown as they would appear in the CS when looking for the target vein. The vein selector is extended into the CS to locate the target vein with puffs of contrast. The sheath and tip of the “Renal” guide remain in the low to mid CS.
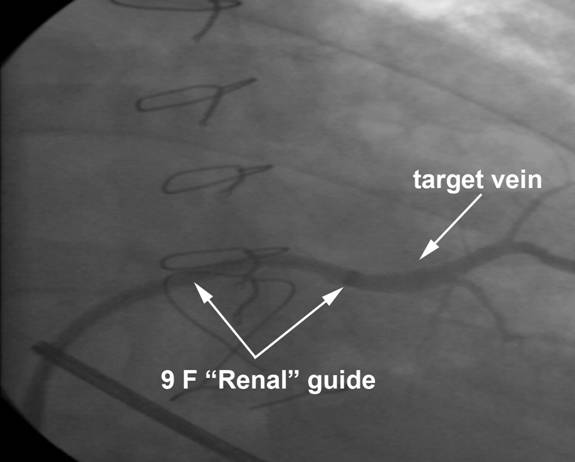
Using puffs of contrast the target vein was located, cannulated with the vein selector and a .014 angioplasty wire was advanced into the vein through the vein selector. The “Renal” LVI-guide was advanced into the target vein using the angioplasty wire and vein selector as a rail (figure 7), the vein selector was removed, retaining the guide wire in the target vessel.
Figure 7 The “Renal LVI guide, vein selector and angioplasty wire are shown in the target vein. The “Renal” LVI guide was advanced out of the sheath over the rail created by the wire and vein selector
Contrast was injected through the “Renal” LVI guide confirming the tip of the guide was in the vein (Figure 8).
Figure 8. Contrast injection through the “Renal’ LVI guide into the target vein confirms the tip of the guide is well within the vein.
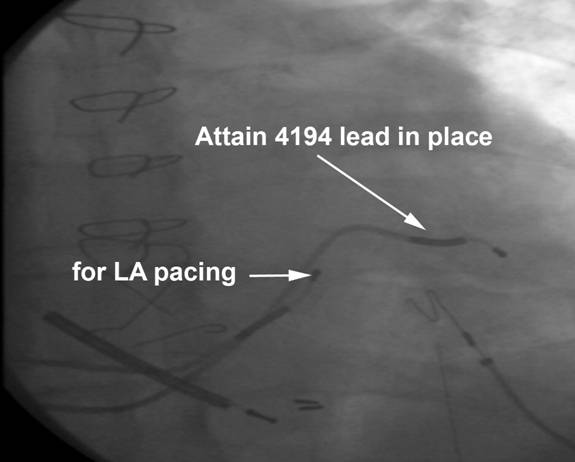
Using the support of the “Renal” LVI guide a 6F bipolar LV pacing lead (Medtronic Attain 4194 OTW) was advanced over the wire into the vein (Figure 9).
Figure 9. The LV lead is in place. The “renal” LVI guide has been cut away and the sheath pealed away. A second Attain lead is in the CS for LA pacing.
The hemostatic hub of the “Renal” LVI was split and the guide removed by slicing. The sheath was then peeled away. The lead was stable without phrenic pacing at 10V, and had a capture threshold of 1.6 volts at .5 milliseconds. The lead was tied down and attached to the generator and the pocket was closed in the normal fashion. The total LV implant time from initiation of CS access to LV lead tie down was 15 minutes, total implant time 25 minutes. Case Report #2
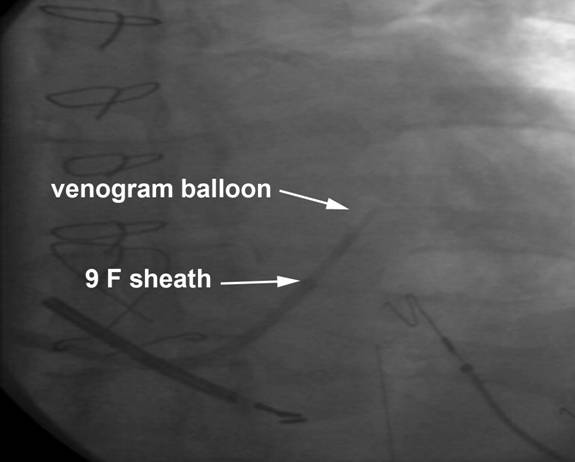
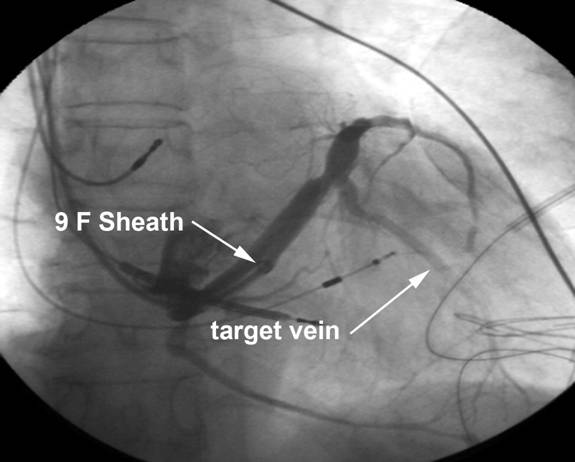
Figure 10. The CS venogram from case 2. The target vein and 9 F sheath are shown.
A 5F vein selector was inserted into the 9F SafeSheath® Worley Telescopic Braided Series Renal Lateral Vein Introducer® (“Renal” LVI guide). (Pressure Products, San Pedro, CA USA). The “Renal” LVI guide with the vein selector was telescoped through the 9F sheath into the CS until the tip of the “Renal” LVI guide was at the tip of the sheath. The vein selector was then advanced out of the Renal” LVI guide into the CS. Using puffs of contrast the target vein was located, cannulated with the vein selector and a .014 angioplasty wire was advanced into the target vein through the 5F vein selector. After the “Renal” LVI guide was advanced into the target vein using the wire and vein selector as a rail, the vein selector was removed, retaining the guide wire in the target vessel (Figure 11).
Figure 11. The angioplasty wire and 9F “Renal” LVI guide are in the target vein. The 9 F sheath is in the CS.
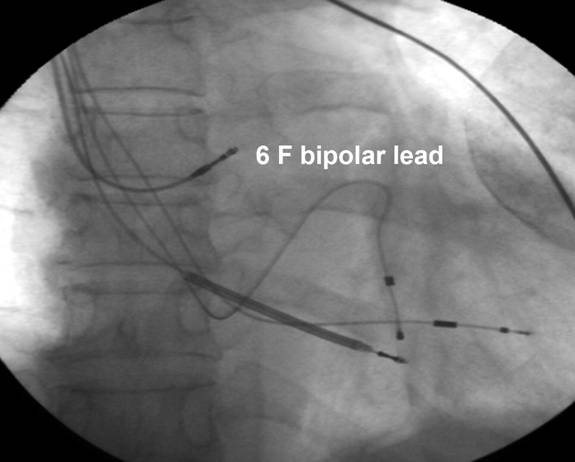
Using the support of the preshaped LVI guide a 6F bipolar LV pacing lead (Quick Site® Model 1056, St Jude Medical) was successfully advanced over the wire into the vein (Figure 12).
Figure 12. The 6 F LV lead is in the target vein.
Discussion The guide-based delivery system used here consists of a 9F ID sheath designed for CS cannulation that provides both the conduit and platform for the 9F OD 7F ID LVI guides (Figure 3). The sheaths and guides provided by the device manufacturers for CS access have an ID of 7F, which does not allow for the insertion of guides large enough to support the delivery of 6F leads. Medtronic’s Attain II catheters are similar in concept to the Pressure Products delivery system but are restricted to the delivery of a 5F unipolar lead (Attain 4193 OTW) that, once positioned, may be less stable than larger leads. Additionally, the unipolar lead provided by the manufacturer’s delivery system does not provide the option of electronic repositioning when needed. The Pressure Products LVI guides are pre-shaped to aid cannulation of the target vein ostium. The lumen of the LVI guide is sufficient to accept both a 6F lead and a .014 in angioplasty wire, and is offered in four pre-shaped curves. In our experience, the renal curve guide provides the support needed for a successful implant in the majority of cases. The compound shape of the renal curve guide places the second curve against the CS when the tip is in the ostium of the vein, which provides additional support for lead delivery. As it is impossible to predict when LV lead placement will be difficult, routine use of guide based delivery systems may reduce overall implant time. Even if a “Renal” LVI guide is used for not used for LV lead placement, the easiest and most reliable way to locate and cannulate the selected target vein with an angioplasty wire is with the use of an appropriately shaped inner catheter referred to here as a vein selector. The device manufacturers provide catheters that can be used as vein selectors, including the 7F Attain I Select® (Medtronic), the 7F CPS AIM® inner catheter (St. Jude Medical), and the 6F Rapido® CS inner catheters (Boston Scientific). The shape of vein selector we find most useful, is the 5F vein selector included with the “Renal” LVI guide. It may be possible to locate and cannulate the target vein with the “Renal” LVI guide alone; however, the most reliable method is to advance it over the rail created by a vein selector and angioplasty wire. (Figure3). After the “Renal” LVI guide is positioned in the vein, the vein selector can be removed, retaining the angioplasty wire in the target vessel. After final LV lead placement, the “Renal” LVI guide is sliced using a cutting device included with the guide and vein selector. The cutting tool is designed to attach to the hub of the sheath, which provides a stable platform during the slicing process. During cutting the LV lead is supported by the sheath, reducing the possibility of lead dislodgement. Removal of the long peel-away sheath used for initial CS access is best performed as follows: 1) before cracking the hub, withdraw the sheath over the lead under fluoroscopy, adding additional slack as needed until the hub reaches the connector; 2) have the surgical assistant squeeze the sheath where it exits the body, in order to compress the walls of the sheath against the lead, securing it in place; 3) when the lead is secure, crack the hub and peel the sheath down to the assistant’s fingers; 4) withdraw the remaining sheath over the lead without peeling; 5) when the lead is free of the sheath, have the assistant securely hold the lead in place and peel away the remainder of the sheath. Conclusion |
| Cardiac Resynchronization Therapy Symposium Home | Instructions | Directors | Opening Speech | Summary | Programme Faculty | Archives | Library | Lectures | Registration | Contact us |
 |